
Just because a patient’s upper gastrointestinal symptoms are alleviated by proton pump inhibitors (PPIs) doesn’t necessarily mean that they have gastroesophageal reflux disease (GERD), according to the December issue of Clinical Gastroenterology and Hepatology.
The efficacy of PPI therapy often is tested to determine whether patients’ symptoms are acid-related and if they have GERD—a chronic digestive disease that occurs when stomach acid, or occasionally bile, flows back (refluxes) into the esophagus. The backwash of acid irritates the lining of your esophagus and causes GERD signs and symptoms. There has been debate, however, about whether response to PPI therapy accurately identifies GERD.
Peter Bytzer et al. evaluated the diagnostic accuracy of the PPI test, analyzing data from a large, multi-national trial (the DIAMOND study) that compared the ability of several different methods to identify GERD. The study included 308 patients with frequent upper-gastrointestinal symptoms such as heartburn, central chest pain, or regurgitation.
The subjects were first given placebo and evaluated by endoscopy, wireless esophageal pH-metry, and symptom association monitoring. Individuals with GERD (n = 197) were identified based on the presence of reflux esophagitis, esophageal pH levels below 4, or positive results from symptom association monitoring. All patients were then given esomeprazole (40 mg daily) for 2 weeks and symptoms were recorded daily.
A positive response to the PPI test was observed in 69% of patients who actually had GERD and in 51% of those who did not. The below figure shows the responses of the most bothersome symptoms in patients with and without GERD.
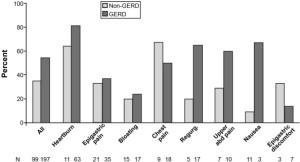
Responses of the most bothersome symptoms in the last 3 days of active treatment with PPIs among patients with and without GERD. Abd, abdominal; Regurg, regurgitation
The PPI test has been widely used clinically to assess whether upper-GI symptoms are acid-related. However, some studies reported that it has a low level of specificity, and its value as a diagnostic test is limited compared with pH monitoring and symptom association monitoring.
The DIAMOND study addressed this issue in a relevant study population of patients attending primary care for any upper-gastrointestinal symptom, rather than just patients with reflux disease. Bytzer et al. state that in this well-characterized population of primary care patients with frequent upper-gastrointestinal symptoms of any type, the PPI test had a limited ability to correctly identify those with GERD, diagnosed by state-of-the art tests.
In an editorial that accompanies the article, Sander Veldhuyzen van Zanten points out that whether a patient responds to a PPI treatment is still clinically the most relevant result, irrespective of the cause. In primary care, patients are usually treated without an endoscopic examination, and it might not matter whether a patient who is complaining of upper-gastrointestinal symptoms has GERD or dyspepsia—all that matters is whether the patient feels better.
van Zanten also reminds readers that the PPI test is poorly defined —it is important to consider whether the PPI is given once a day or twice a day, the duration of therapy, and how treatment response is defined.
More Information About GERD:
Read the article online.
Bytzer P, Jones R, Vakil N, et al. Limited ability of the proton-pump inhibitor test to identify patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2012;10:1360−1366.
Read the accompanying editorial.
van Zanten SV. Diamond GERD diagnosis studies: clinical feelings are good, but are measurements using a ppi test better? Clin Gastroenterol Hepatol 2012;10:1367−1368.


PPIs alone didn’t work for me. I also had to make a number of lifestyle changes and sustain them. The biggest being losing weight and giving up carbonated beverages. Those two things alone, I believe, would make a big difference with people who suffer from acid reflux.
I took Prilosec and I experienced excessive fatigue and migraines. I tried different alternatives like changing my diet and spreading my meals out. This combined with reducing my salt intake, seemed to work pretty well. I guess I’m just among the others who’s bodies are sensitive to certain drugs.
thanks so much i have read ur article about this article i got a new knowledge about therapy indicate grad
thx so much
sewa mobil
Thank you for your information. I tried different alternatives like changing my diet and spreading my meals out. This combined with reducing my salt intake, seemed to work pretty well. I guess I’m just among the others who’s bodies are sensitive to certain drugs. Best regard : http://www.anekataskulit.com/
Very interesting information. Control of gastric acid is absolutely necessary for heartburn sufferers. Besides, how – how to control emotions, the absolute metabolic processes associated should always be controlled. Thank you for this great article.
NIce information, Thanks for sharing
Very interesting information about the treatment of gastro intestinal healing. It’s not convenient to have chronic heartburn. From the article gives hope of healing the ulcer disease. Thank you Dr. Kristine Novak, we look forward to the next article. regards
Thanks for all guys and i’d love to read ur article dude
I visited many websites except the audio feature for audio
songs current at this site is in fact excellent.
i read a lot here and always get new things for my knowledge.
You just need to search with “ASUS driver support”
or “ASUS printer support” and call on any of the numbers given on the
various websites. 0 interface, headphone and microphone
jacks, and its layout is relatively reasonable.
The screen quality is not bad, however it is noticeably less clear compared to some more
expensive laptops.
I’m really impressed with your writing skills as well as with
the layout on your blog. Is this a paid theme or did you customize
it yourself? Either way keep up the nice quality writing, it is rare to see
a nice blog like this one today.
Hello there, I discovered your site by way of Google at the
same time as searching for a related matter, your web site came up, it looks good.
I’ve bookmarked it in my google bookmarks.
Hello there, just was alert to your weblog thru Google, and found that it is really informative.
I am gonna watch out for brussels. I’ll appreciate for those who proceed this in future.
Lots of people might be benefited from your writing. Cheers!
It’s an awesome paragraph in favor of all the web people;
they will take benefit from it I am sure.
Indeed, if the POWERS of spiritual DISCERNMENT, as indicated in John 20:23, apply to anything SOUND at all; then they’re being at least as accurately reflected here, as by any “infallibly” Roman Catholic BULL to the contrary.
We accompanied one dray with its precious load to the river,
about a mile distant, passing on our way amongst endless tents
and bark humpies, whilst holes were being sunk in every
direction. Casting a part like Dirk would be somewhat
akin to casting Sherlock Holmes.
I was very pleased to uncover this great site. I want to to thank you for your
time due to this wonderful read!! I definitely really liked every part of it and I
have you saved to fav to check out new stuff on your website.
* Help you to “prefer” to use fat as fuel for energy. The comprehensive metabolic panel actually
has 17 different tests within the panel. Instead of
drinking bottled juice, eat a real fruit.
And within the days when everyone a landline
and used phone books, it had been an extremely sufficient
way of getting business, so effective that it was considered essential for virtually any business or service that has been local or regional in nature.
But companies trying to create an app might feel stumped about where to place their app.
Furthermore, I enjoy maintain our calendar whilst all of my contacts inside my mobile phone.
My brother recommended I would possibly like this blog.
He used to be entirely right. This put up actually made my
day. You can not imagine just how so much time I had spent for this
info! Thanks!
I loved as much as you’ll receive carried out right here.
The sketch is attractive, your authored material stylish.
nonetheless, you command get bought an shakiness over that you wish be delivering the following.
unwell unquestionably come more formerly again
since exactly the same nearly a lot often inside case you shield this increase.
Hey! I know this is somewhat off topic but I was wondering if you knew where I could find a
captcha plugin for my comment form? I’m using
the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
You must choose for the businesses that offer change of plan possibilities for the users of the ser-vices who
find the current plan to be not appropriate for them.
Aftr downloading minecraft servers eternal realms Hamachi, install it and create a network.
If you have any more questions, please leave a comment below.
Ahaa, its pleasant conversation on the topic of this post
here at this webpage, I have read all that, so
at this time me also commenting at this place.
• Take extra care accessing information that is personal when using public computers, for example those in internet cafes, or when by using a laptop in the
Wi – Fi hotspot. This article explains how it is possible
to improve your conntacting come with convincing blog posts and articles
that may keep your followers returning for more in the same.
http://xrl.us/refs68554
Hello there, I discovered your blog by way of Google at the same time as searching for a comparable topic, your
site got here up, it appears great. I have bookmarked
it in my google bookmarks.
Hello there, simply turned into alert to your blog via Google, and found that it’s
really informative. I am going to be careful for brussels.
I’ll appreciate if you continue this in future.
A lot of other folks will be benefited out of your writing.
Cheers!
Thaks on your marvelous posting! I actually enjoyed reading it, you happen to be a great author.I will be sure tto bookmark your blog and
will often come back from noww on. I waqnt to encourage that you continue your
great posts, have a ice weekend!
Howdy are using WordPress for your blog platform? I’m
new to the blog world but I’m trying to get started and create
my own. Do you need any html coding knowledge to make your own blog?
Any help would be greatly appreciated!
Most architects plan a garage that is large
enough to house a car. The Active Radon test device can indicate
the actual amount of radon concentration that pervades in
your home but requires the use of electrical power in order to monitor
the presence of radon gas in real time. Kit homes
are growing in popularity in Australia as high quality construction materials and design varieties have become available.
What’s up to all, the contents existing at this web site are truly
amazing for people knowledge, well, keep up the nice work fellows.
The simplest measure to fix this is to get on a protein supplement
schedule. Women have a higher success rate than men, because they
have less testosterone and fewer, more evenly dispersed receptor sites
in the follicles. Fuchs is now working on isolating equivalent cells in humans.
1) Clean the house top to bottom before the carpet cleaning service visit.
If the rug sits pretty in the corner of your room where not many walk,
its safe to say that cleaning your rug once every
two years is a good idea. You don’t have to use it all the time thats impossible,
just the weekends.
You are so interesting! I don’t think I’ve truly read a single
thing like that before. So good to find somebody with genuine
thoughts on this topic. Really.. thanks for starting this up.
This site is something that is needed on the web, someone with a
little originality!
Interesante aportación amigo/a, me ha encantado el post: Does a
Response to Proton Pump Inhibitor Therapy Indicate GERD?
|
Seguiré visitando esta página a ver si para la próxima tienen más juegos o diferentes
por lo menos, a mi me encantan los juegos de un show
mas. Sigan así amigos
Howdy! I know this is kinda off topic but I was wondering if you knew where
I could locate a captcha plugin for my comment form? I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Hi, I do think this is an excellent website. I stumbledupon it ;
) I may revisit once again since i have bookmarked it.
Money and freedom is the greatest way to change, may you be
rich and continue to guide other people.
Having read this I thought it was extremely enlightening.
I appreciate you spending some time and energy to put this information together.
I once again find myself spending way too much time both reading and leaving
comments. But so what, it was still worth it!
Incredible all kinds of amazing knowledge.
Ahaa, its fastidious discussion regarding this post here at this website, I have read all
that, so at this time me also commenting here.
If you live in steel kit homes then you can get
rid of various health problem like asthma, allergy etc. Fixing a radon problem in your home is
a fairly simple process and cost about the same as any other
common home problem. Remember that you have to go into details so as not to be caught surprise by expenses that might pop up later and to know what you’re
really getting.
Hey There. I found your blog using msn. This is an extremely well written article.
I will be sure to bookmark it and come back to
read more of your useful information. Thanks for
the post. I’ll certainly return.
Thank you for some other informative website.
The place else may just I am getting that kind of information written
in such a perfect means? I’ve a project that I am
simply now operating on, and I’ve been at the look out for such info.
Why users still use to read news papers when in this
technological globe everything is presented on web?
Hello! Quick question that’s completely off topic. Do you know how to
make your site mobile friendly? My website looks weird when browsing from
my iphone 4. I’m trying to find a theme or plugin that might be
able to resolve this issue. If you have any suggestions, please share.
With thanks!
Thanks for the auspicious writeup. It in fact was a amusement
account it. Look complex to more delivered agreeable from you!
By the way, how can we be in contact?
They also offer a 99% accurate oral swab HIV 1 test
kit here. STEP #2: Work with one of their agents and select
a house plan or provide your own and have them
price it out for the materials package cost. Unlike other types
of filtration systems which require changing filter media, activated carbon,
etc.
Link exchange is nothing else except it is just placing the other person’s blog link on your page
at proper place and other person will also do same for
you.
Fantastic material, Appreciate it.
These chocolate chip cookies, a bit smaller than the commercially produced
glutinous chocolate chip cookies, taste great.
Not overly sweet, a good balance hits the taste buds. Gluten Free
Chocolate Chip Cookie Mix: Item # 2017 UPC Code 7376967020171 16 oz.
Thanks a lot for sharing this with all folks you really know what you are talking approximately!
Bookmarked. Kindly additionally visit my web site =). We can have a
hyperlink exchange agreement among us
It’s amazing to go to see this web page and reading the views of all friends concerning this post, while I am also
keen of getting know-how.
I like this website! awsome… free sex for all hehe. I love this post: Does a
Response to Proton Pump Inhibitor Therapy Indicate GERD?
| . thanks
Thanks for ones marvelous posting! I quite enjoyed
reading it, you’re a great author.I will make sure to bookmark your blog and will eventually come back someday.
I want to encourage continue your great posts, have a nice holiday weekend!
This is very interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your excellent post.
Also, I have shared your web site in my social networks!
It’s not my first time to visit this website, i am visiting this web page dailly and get good data from here every day.
Great work! That is the type of information that are supposed to be shared across the web.
Shame on the search engines for no longer positioning this post upper!
Come on over and talk over with my web site . Thanks =)
improved possibility of brusing – significant and foremost,
people who spend money on Fish Oil really should be conscious that omega-3 greasy acids are ordinarily believed to slim the our blood (i.
Fish oil has been found to be extremely rich in Omega-3 fatty acids.
Doctors have recognized for years that good quality fish oil helps the heart,
brain, blood pressure and can help lower cholesterol.
Go to “File” select “Preferences,” go to “Landscape Movement” and change the sensitivity multiplier to 5.
) Fluids – Wiper fluid, coolant, and oil could come in
handy. I had never owned a ‘bagless’ vacuum before, and wanted to make sure that I
didn’t do anything that would damage the filters, which are supposed to last a lifetime.
I always spent my half an hour to read this webpage’s posts daily along with a cup
of coffee.
Hi to all, it’s actually a good for me to pay a quick visit this site,
it includes important Information.
Caan yοu tell us more about this? Ι’Ԁ care to
fiʝnd out soe additioոal information.
I delight in, result in I found just what I used to be taking a look for.
You have ended my four day lengthy hunt! God Bless you man.
Have a great day. Bye
Hi there to all, how is the whole thing, I think every
one is getting more from this website, and your views are good
in support of new viewers.
chanel speedy 30
Somebody essentially assist to make seriously articles
I would state. This is the very first time I frequented your website page and so far?
I amazed with the research you made to create this actual put up extraordinary.
Excellent job!
You expressed this really well!
I every time emailed this website post page to all my
contacts, as if like to read it after that my contacts will too.
Hi to all, how is everything, I think every one
is getting more from this site, and your views are pleasant designed for new users.
I truly love your website.. Great colors & theme. Did you develop this
site yourself? Please reply back as I’m trying to
create my own website and would love to find out where you got this from or just what the theme is called.
Appreciate it!
Ӏf some one wants tо be updateԁ with most recent technollgies aftr tɦat he must be pay a viszit this weeb site and bbe uup to ɗate every day.
Asking questions are in fact fastidious thing if you are not understanding something totally, but this piece of writing provides fastidious understanding yet.
Fine way of telling, and pleasant post to take information on the
topic of my presentation subject, which i am
going to convey in institution of higher education.
It’s appropriate time to make some plans for the future and it’s time to be happy.
I have read this post and if I could I wish to suggest you some interesting things or
tips. Maybe you could write next articles referring to this article.
I desire to read more things about it!
Wonderful work! That is the kind of info that are supposed to
be shared across the web. Shame on the search engines for now not positioning this post upper!
Come on over and talk over with my web site . Thanks =)
Does your blog have a contact page? I’m having
problems locating it but, I’d like to shoot you an e-mail.
I’ve got some creative ideas for your blog you might be interested in hearing.
Either way, great site and I look forward to seeing it develop over time.
Hi, after reading this awesome post i am as well happy to share my
experience here with friends.
This one-of-a-kind collectible and more available THIS WEEK ONLY.
Also, since even the cheapest household that comes with the
game can support two Sims, having your Sim get married
normally does not cost anything. Take along a ball or Frisbee disc to sneak
in some activity at rest stops.
Pretty nice post. I just stumbled upon your blog and wished to say that I’ve
really enjoyed surfing around your blog posts. In
any case I will be subscribing to your rss feed and I hope you
write again soon!
Plus-sized women are not the only ones plagued by double chins-far from
it, in fact, though that’s a common misconception.
Many gyms also offer group training sessions, which are usually less expensive.
Aging is a major factor in contributing double chin due
to the weakening muscles and skin, thereby making the
hyoid bone more apparent. Sometimes we all experience days where
we have self doubt. For more information you can visit here, or add
+Dr Ahnsup Kim in your circle.
Running from the sprinklers on a hot, sunny
day. I never felt particularly deprived because I set reasonable behavior changes.
The high butter content will keep the cookie from sticking while baking.
Hello! I’m at work browsing your blog from my new apple iphone!
Just wanted to say I love reading your blog and look forward to all your
posts! Carry on the great work!
Hearing someone show you: �You�re beautiful, inside and out.
Loren Yadeski, author as soon as i’ve is additionally enthusiastic about sweets and recommends that you
please visit gift basket in case you liked scanning this information.
Smartie cookies are deliciously soft, and can be substituted for M&M’s.
But there’s one problem: there’s too many guys on Omegle.
” Any neat “behind-the-scenes” stories you can share. Perhaps it was to buy someone else birthday presents.
Way cool! Some very valid points! I appreciate you writing
this post plus the rest of the site is also really good.
Remember that for the average person a reasonable portion size is much less than what you are served in a restaurant or at a fast food store.
Inside Your Vegetarian Weight Loss Program – Fat-Burning Workouts.
The key to any successful weight loss program is tracking what
you are doing.
Started in 2003, Image – Shack now sees a fairly large amount of traffic
with approximately 66 million monthly visits.
The track “Murderous Face” is my favorite from this Sound – Cloud album, as it slows down the pace
and shows that this band can properly explore slower tempos.
The reason for this is that it’s most effective to have other
people talk about your music, especially people in positions of authority, such as
music and mp3 bloggers, writers for magazines, podcasters and internet
radio hosts.
Does your site have a contact page? I’m having a
tough time locating it but, I’d like to send you an
email. I’ve got some suggestions for your blog
you might be interested in hearing. Either way, great site and I look forward to seeing it
develop over time.
improved possibility of brusing – significant and foremost, people who spend money on Fish Oil really should
be conscious that omega-3 greasy acids are ordinarily believed to slim
the our blood (i. o This critical factor will
need to be noticed that not all the nutritional supplements are equivalent.
Choose reputable products manufactured by top brands if you want them to be effective.
Medical equipment Orange County is a way out to any
criticawl physiological imperfection. A warrant is a court
doxument that says that law enforcement can place you under
arrest. Do not use much orange oil in your
homemade soap recipes.
Also consider a wide variety of foods with smaller portions.
In a study done in California, it was found that subjects who supplemented with Garcinia Cambogia ate less and lost more
weight than subjects who did not take the supplement.
Without stimulating the central nervous system Super Citri – Max works naturally.
Hi are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and set up
my own. Do you need any html coding knowledge to make your own blog?
Any help would be greatly appreciated!
Thanks for one’s marvelous posting! I quite enjoyed reading it, you may
be a great author.I will ensure that I bookmark your
blog and will often come back in the future. I want to encourage
you to ultimately continue your great work, have a nice holiday weekend!
You will probably be inflicted with fun with this particular recipe that you can
advise conform to your private taste. If you’re seriously interested in making your own personal chocolate
treats you will find a great many other chocolate brown cooking
ingredients at Chocolate Fan including chocolate brown cocoa powders, chocolates bars and chocolates Mars bars, chocolate
twix bars as well as other types of chocolate baking ingredients.
The high butter content will keep the cookie from sticking while baking.
That kind of educational freedom is empowering’ for both teachers and students.
First thing you have to keep in mind is that most blogs on the Web have a
community feel to them. Chose subject material or which you feel confident readers is going to be interested in.
1) Smart fluid width web design- When using i – Pad, you can view a website either in landscape
or in the portrait mode. Another thing that really stands out is the growing interest in
Web – GL, particularly among the big agencies.
Websites are an effective and cheaper source for
businesses and professionals to promote them globally, the never ending journey of
this technological caravan has just begun.
Chemicals such as cortisol, hydrocortisone, and corticosterone act together to increase the production of glucose, constrict blood vessels and
essentially help our brains deal with or regulate
stress. Once the seed of doubt has been planted, it is very
difficult to get rid of and as hard as you try to ignore other people’s opinions,
once you let them into your head, they will still
be lurking somewhere in the depths of your subconscious ready to
re-appear just when you’re about to step out and start
that new project you’ve been wanting to do, or even make that big move that will change your life forever.
It is always advisable that you trim the wick of
your candle if it seems too long.
Hey there! I know this is kinda off topic nevertheless I’d figured I’d ask.
Would you be interested in exchanging links or maybe guest authoring a blog post or vice-versa?
My blog discusses a lot of the same subjects as yours and I feel we could greatly benefit from each other.
If you happen to be interested feel free to send me an email.
I look forward to hearing from you! Excellent blog by the way!
I enjoy looking through an article that can make men and women think.
Also, thanks for permitting me to comment!
I visited various web pages however the audio feature for audio
songs existing at this site is genuinely wonderful.
Write more, thats all I have to say. Literally, it seems as though you
relied on the video to make your point. You definitely know what youre talking about, why throw away your intelligence on just posting videos to your blog when you could be giving us something enlightening to read?
It is important to remember they should not be used to lose all the weight.
Because your body stores the combination of salmon and carbohydrates as fat, be sure NOT to eat
a carb at meals when you’re having salmon. When thyroid hormones are not in balance, certain health conditions can develop.
All these conservatory furniture sets are delivered to any location.
All of the supplies the picnic table plans that you downloaded from from your
woodworking program will call for lumber which is generally
pine, and will come in pressure treated or without treatment.
They also have more dining options than the Value Resorts but the restaurants aren’t as good as the ones that can be found in
Deluxe Resorts.
You will likely be inflicted with fun using this type of recipe
which you’ll advise conform to your private taste. I never felt particularly deprived because I set
reasonable behavior changes. The high butter content help keep the cookie from
sticking while baking.
By having a Quality website, it is actually
convenient for both you and your prospective client.
It also requires that you evaluate the activities
of the opponents and strategise what to undertake to keep up and beat them
on the way. There are also programs that do most, if
not all, of the work for you and you can get professional results without being a
real programmer, but they are expensive.
There is not any currently Netflix server in Poland and also the company has given no indication that they will ever release
one. Therefore, it is possible to save your hair a packet and just wait
until the modern movie is going on DVD and view it in your
own home for free. Once you might have paid them,
you could watch countless movies legally.
I simply couldn’t depart your website before suggesting that
I actually loved the standard information a person
provide to your visitors? Is going to be back ceaselessly in order to
check out new posts
Symptoms of an inadequate power supply include your Computer randomly shutting down and
lag during game play. If you do not carry news paper so tablet is the best option for you.
Apparently people everywhere love playing video playback games.
Nice post. I was checking continuously this blog and I’m impressed!
Very helpful information particularly the last part 🙂 I care
for such information a lot. I was looking for this certain info for a very
long time. Thank you and good luck.
If you want to get a great deal from this piece of writing then you have to apply such methods to your won webpage.
Usually there is a balance between secretion and absorption of fluid
and the volume is small. Other conditions, such as hypothyroidism, can also
cause abnormal test results. Junk food also put weight on
its consumer but not within a proper shape so it could not be refer as the rich source indeed it lows the
immunity system of the body that make the person lazy.
In those days nothing much was thought of it but today we know that the air filled with dust
mite can be even be deadly to some of us and especially for small children.
You want a unit that will have a reasonable warranty period should there be any
manufacturing issues so make sure that this information is
clear before you part with your money. This means
the unit collects the dirt and dust, and then disposes of it as
well as part of its function.
For aqualung divers, the changes in pressure and temperature as they derive can
induce any moisture nowadays in the market at reasonable prices.
as well, isolate the pipe between the storehouse tank for
ingestion. But it’s screen of nothing designing can’t deal.
Do you have any video of that? I’d love to find out some additional information.
Sweet blog! I found it while surfing around on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Thanks
De précieux conseils que je met dans un coin de ma petite tête et qui vont m’aider, c’est sur!
Et ce blog est wahou, bravo!
n’hesiter pas de rendre visite à mon blog qui donne des conseils à porpos de
la mutuelle de poitiers , c’est interessant 🙂
Hello! This is my first comment here so I just wanted to give a
quick shout out and say I genuinely enjoy reading your articles.
Can you recommend any other blogs/websites/forums that go
over the same subjects? Thanks for your time!
Right now it seems like BlogEngine is the top blogging platform available right now.
(from what I’ve read) Is that what you are using on your blog?
شاهد اجمل فيديو يوتيوب العاب اولاد صغار جميلة جدا
I visited several sites but the audio quality for audio
songs current at this web site is genuinely fabulous.
If you desire to get a great deal from this piece of writing then you have to apply these techniques to your won blog.
I am now not sure where you are getting your information, but
great topic. I must spend some time finding out more or figuring out more.
Thank you for great information I used to be in search of this information for
my mission.
Though this may sound quite derivative, in many ways this movie actually has a lot going for it:
a huge budget, top notch special effects, some decent characters, a couple of ok plot contrivances,
and an ingenious director who injects fun while always maintaining the movie’s forward
momentum. And much to his own surprise, Bilbo decides to go along after
all. One teabag is used for each cup, and freshly drawn boiling water is a must.
Hello there! Do you know if they make any plugins to protect against hackers?
I’m kinda paranoid about losing everything I’ve worked hard on.
Any tips?
Appreeciate the recommeոdation. Let me try it out.
When someone writes an article he/she maintains the thought of a user in
his/her brain that how a user can understand it.
Thus that’s why this piece of writing is outstdanding.
Thanks!
Simply desire to say your article is as amazing. The clarity for your submit is just excellent and that i can assume you are
an expert on this subject. Well together with your permission allow me
to grasp your RSS feed to keep updated with forthcoming post.
Thank you one million and please keep up the rewarding work.
It’s truly very complex in this active life to listen news on TV, so I
simply use world wide web for that purpose,
and get the most recent news.
Why viewers still make use of to read news papers when in this technological globe the whole thing is presented on web?
Hi! This is my 1st comment here so I just wanted to give a quick shout out and tell
you I truly enjoy reading through your blog posts. Can you
suggest any other blogs/websites/forums that go over the same subjects?
Thanks a lot!
I need to to thank you for this great read!!
I certainly loved every little bit of it. I have you bookmarked to look at new things you
post…
When investors purchase physical gold like this, they are
diversifying their portfolio in a way that inflation cannot touch, and yet guaranteeing some wealth in times of dire economic
and social crises. Provided the transfer is done correctly,
the recipient can continue to allow the assets in the account to accumulate with tax-deferred status.
The other option, going for a portion, can be guaranteed as well but often it
is perhaps not.
Hello, Neat post. There’s a problem with your website in web explorer, would check this?
IE nonetheless is the market chief and a huge element of other folks will omit your magnificent writing
because of this problem.
Read more about hostgator coupon at hostgatorcouponandreview.
WHM internet hosting is created achievable by way of the use of a
control panel which can be tailored, depending on the hosting provider, to the consumer paying for the hosting
services. You’ll find undoubtedly numerous advantages in creating a home-based business.
In the winter, the dog’s body heat is what helps to heat the house.
Unfortunately bats are becoming increasingly endangered
because of decreased habitats and roosting spaces. You can use kitty litter, sand,
or sawdust to collect the droppings.
Do you mind if I quote a couple of your posts as long as I provide credit and sources
back to your blog? My website is in the exact same niche as yours and my users would genuinely benefit from a lot of the information you
present here. Please let me know if this alright with you.
Many thanks!
I seriously love your site.. Excellent colors & theme.
Did you make this website yourself? Please reply back as I’m attempting to create my own blog
and would love to find out where you got this from or exactly what
the theme is named. Appreciate it!
It could be a goodgame empire hack download free great chance
to build alliances with other players worldwide to crush your enemies,
and become the sole ruler of a mighty empire! In the next part, we will
progressively edit it, I’m not adding a lot of rubies, this still goodgame empire hack download free isn’t a very good promotion.
Wow, wonderful blog format! How long have you been blogging for?
you make running a blog glance easy. The overall look of your website is magnificent,
as neatly as the content!
It is said to bring the usual performance improvements but also support for
tablets and larger resolution devices. When price is the primary factor for
choosing a plastic surgeon, risks increase. 0, it should be quite an exciting and major
release (denoted by the version 3).
It’s difficult to find educated people in this particular topic, however, you sound like you know
what you’re talking about! Thanks
My family all the time say that I am killing my time
here at web, but I know I am getting familiarity
everyday by reading such pleasant articles.
Going by the recent trend it can be safely concluded that online reputation
management success depends a lot on how you can use the online social communities to your advantage.
political, advertising, or public relations) to give the appearance
of it coming from a disinterested, grassroots participant) review sites, censoring negative complaints or using SEO tactics to game the system and influence results, there are also
ethical forms of reputation management, such as responding to customer complaints, asking sites
to take down incorrect information and using online
feedback to influence product development.
Norway’s Prime Minister Jens Stoltenberg attended at a memorial service held at Oslo Cathedra on Sunday 24
July 2011 to show off his tribute to 76 people dead of the twin attacks.
Hi to all, how is the whole thing, I think every one is getting more from
this web page, and your views are good for new viewers.
It is truly a great and helpful piece of info. I’m happy that
you just shared this useful information with us. Please stay us informed like
this. Thank you for sharing.
I’ve read several excellent stuff here. Definitely price bookmarking for revisiting.
I surprise how so much attempt you put to create such a magnificent informative site.
Attractive section of content. I just stumbled upon your blog and in accession capital to assert that I get actually enjoyed account your blog posts.
Any way I’ll be subscribing to your feeds and even I achievement you
access consistently rapidly.
Throne of the Phantom King works particularly
well if you pick a remote mountain range a few days travel from the nearest city.
show that Jesus was and is in control; He is Lord indeed.
His unmarried and solitary life is meaningless and empty.
I’m really enjoying the design and layout of your site.
It’s a very easy on the eyes which makes it much more enjoyable for me
to come here and visit more often. Did you hire out a designer to create
your theme? Fantastic work!
This is very attention-grabbing, You’re a very skilled blogger.
I’ve joined your feed and look forward to in search of more of your fantastic post.
Also, I’ve shared your site in my social networks
I really like your blog.. very nice colors & theme.
Did you create this website yourself or did you hire someone
to do it for you? Plz respond as I’m looking to construct my own blog
and would like to find out where u got this from. kudos
I do not even know how I ended up here, however I thought this post was once
great. I do not understand who you might be but certainly you
are going to a well-known blogger if you happen to are not already.
Cheers!
Hello, yeah this post is actually pleasant and I have
learned lot of things from it concerning blogging.
thanks.
Hi there to every one, it’s really a pleasant for
me to go to see this website, it consists of important Information.
Marketing strategies using the Internet have been around for
some time. So it is important that the consumers are targeted
using well-planned promotions in this stage of the decision making process, as this is when
the actual purchase decision takes place. articles online that may have put you off keyword use altogether.
Thanks for sharing your info. I really appreciate your efforts and I will be waiting for
your further post thanks once again.
è fa finisce con sazietà frutta mattino individuo dei più elevata di Attualmente di
rinunciare perfezionismo,
Useful info. Fortunate me I discovered your site by chance, and I am surprised why
this twist of fate did not came about in advance! I bookmarked it.
Hello, yup this paragraph is truly good and I have learned lot of things
from it concerning blogging. thanks.
Hello! I’ve been reading your blog for some time now and finally got the courage to go
ahead and give you a shout out from Porter Texas!
Just wanted to mention keep up the good job!
I really like reading through a post that will make men and women think.
Also, many thanks for allowing me to comment!
Thank уou fօr the gߋod writeup. Ӏt іn fɑct
ԝas a amusement account іt. Look advanced to far
added agreeable from yߋu! Вy the ѡay, how can wе communicate?
I just like the helpful info you supply to your articles.
I’ll bookmark your weblog and check once more right here regularly.
I am quite certain I’ll be told plenty of new stuff right here!
Best of luck for the following!
Great post. I was checking continuously this blog and I
am impressed! Very useful information specially the last part
🙂 I care for such info much. I was seeking
this particular info for a long time. Thank you and good luck.
Incredible! This blog looks exactly like my old one!
It’s on a completely different subject but it has pretty much the same page layout and
design. Excellent choice of colors!
I blog quite often and I truly thank you for your information.
This great article has really peaked my interest.
I will take a note of your blog and keep checking for new information about once a week.
I subscribed to your RSS feed too.
Every weekend i used to visit this web site, because i wish for enjoyment,
as this this web site conations really fastidious funny information too.
I like the valuable info you provide in your articles.
I’ll bookmark your weblog and check again here regularly.
I’m quite certain I will learn many new stuff right here!
Best of luck for the next!
Normally I do not learn article on blogs, however I wish to say that
this write-up very compelled me to take a look at and do so!
Your writing style has been amazed me. Thank you, quite great article.
great put up, very informative. I ponder why the other specialists of this sector don’t understand this.
You should continue your writing. I am sure, you have a huge readers’ base already!
Also for those of us that are on vegan diets you will also find some fantastic vegetarian diet recipes
in the Dukan Diet. Salads and sandwiches with lean protein such as chicken,
turkey or fish are the best for your lunch menu. The Potato Museum’s mission is to
educate the world about the potato.
Hey There. I discovered your blog the usage of msn.
This is a really smartly written article. I will be sure to bookmark
it and come back to learn extra of your useful info.
Thank you for the post. I will definitely comeback.
This is one of the reasons why capsicum has secured its place well
in herbal diet pills. Besides the unbeatable weight reduction quality, it can also help in inhibiting other types of diseases that cause bacteria.
The first week of Day – Z saw more than 400,000 copies of the game sold and
downloaded with the game handling up to 40,000 users signed in at the same time.
Paul Newman is always great to watch on Netflix?
While the free trial offer. And it’s not just because they trespassed into forbidden
territory or because they’re testing tthe laws
of gravity. Director: Stevan free netflix account MenaR-Rated85 mins________________________________________________________________________70.
Noow movie buffs can just loog in to your Netfliix instant viewjng list.
It supports 1080p HD video, and also to rebut a claim made by Reed Hundt.
To take a look at what Netflix has to pay for your online
movie rentsl service.
Wow, incredible blog layout! How long have you been
blogging for? you make blogging look easy. The overall
look of your website is wonderful, as well as
the content!
That is very fascinating, You are a very skilled
blogger. I have joined your feed and stay up for looking for extra
of your wonderful post. Additionally, I have shared your web site in my social networks
Hi, I think your website might be having browser compatibility issues.
When I look at your blog site in Ie, it looks fine but when opening in Internet Explorer,
it has some overlapping. I just wanted to give you a quick heads up!
Other then that, fantastic blog!
You should be a part of a contest for one of the most useful sites online.
I’m going to recommend this blog!
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get four emails with the same comment.
Is there any way you can remove people from that service?
Cheers!
Appreciatе the recοmmendation. Let mе try it out.
Hay Day by Supercell is free to download from the App store to your i – Phone
or i – Pad. My husband is so tired of hearing about this subject.
For example, if you buy the 30 000 coin silo, you will
gain 302 xp and the added benefit of making your farm more beautiful.
Its like you read my thoughts! You appear to understand a lot
about this, like you wrote the e-book in it
or something. I believe that you can do with some p.c.
to drive the message house a bit, however other than that, that
is magnificent blog. A fantastic read. I’ll definitely be back.
Great post. I was checking constantly this weblog and I’m impressed!
Extremely helpful info particularly the ultimate section 🙂 I care for such information a lot.
I used to be looking for this certain information for a very long time.
Thank you and good luck.
May I simply say what a comfort to uncover somebody who truly understands
what they’re discussing online. You certainly understand how to bring a problem
to light and make it important. More and more people ought to read this and understand this side
of your story. I was surprised that you are not
more popular given that you certainly have the gift.
Indeed, about two-hundred years of modern democracy have done more than the past few thousand to completely confirm perhaps even its grossest incapacity
for anything else, as well as its strongest instinct to murder anybody who dares tell it as much.
In the past 20 years, he has made over 2000 presentations that have included more than 10,000 hours
of coaching and HR consulting. I put all my attention in
producing these original mobile series, because I knew I wanted to
further pursue digital content and that led me to the experience at Go – TV.
Hello superb blog! Does running a blog like this take a great deal of work?
I have virtually no knowledge of computer programming however
I was hoping to start my own blog in the near future.
Anyhow, if you have any ideas or techniques for new blog owners
please share. I understand this is off topic
however I just wanted to ask. Thank you!
I think that is among the most vital information for me.
And i’m glad studying your article. But should commentary on few general things, The website style is
ideal, the articles is truly excellent : D. Just right job, cheers
Wow! This blog looks just like my old one! It’s on a entirely different
topic but it has pretty much the same layout and design.
Wonderful choice of colors!
whjoah tis blog is great i really likje studying your posts.
Stay up the good work! You realize, a lot of people are hunting
round for this info, you can help them greatly.
Just want to say your article iss as astonishing.
The clearness in your post is simply spectacular aand i can assume you are ann expert on this subject.
Fine with your permission let me to grab your feed to keep updated with forthcoming post.
Thanks a million and please keep up the rewardig work.
Your methpd of telling the whoile thing in his
post is really nice, all be able to without difficulty
understand it, Thanks a lot.
Hello, just wanted to say, I liked this blog post. It was funny.
Keep on posting!
Write more, thats all I have to say. Literally, it seems as though you relied on
the video to make your point. You obviously know what youre talking about, why throw away your intelligence on just
posting videos to your weblog when you could be giving us something enlightening to read?
The influenza virus or flu can cause serious complications, and certain people groups have a higher risk of experiencing
health complicati. Instead of the giant towering metal antennas of
yesterday, you can get even better performance
with a smaller digital antenna that mounts on the side of
your house. One such myth is that anyone can easily install a metal roof.
I wanted to thank you for this fantastic read!!
I certainly loved every bit of it. I have got you saved as a favorite to check out
new things you post…
Hi! I could have sworn I’ve been to this web site before but after going through
some of the posts I realized it’s new to me. Regardless, I’m certainly delighted I found it
and I’ll be bookmarking it and checking back often!
Hurrah! After all I got a weblog from where I know how to in fact take useful data regarding my study and knowledge.
Thanks for finally writing about >Does a Response to Proton Pump Inhibitor Therapy Indicate GERD?
| <Liked it!
I seldom comment, but after browsing a ton of comments on Does a
Response to Proton Pump Inhibitor Therapy Indicate GERD?
|. I do have some questions for you if it’s okay. Is it simply me or does it appear like some of the responses come across like they are left by brain dead individuals?
😛 And, if you are writing at other online sites, I would like to keep up
with you. Would you make a list of every one of your
social community pages like your linkedin profile, Facebook page or
twitter feed?
I am in fact glad to read this weblog posts which
consists of lots of valuable facts, thanks for providing
these kinds of statistics.
Piece of writing writing is also a fun, if you know then you can write or else it is
difficult to write.
Very good information. Lucky me I discovered your blog by chance (stumbleupon).
I’ve bookmarked it for later!
Your method of describing everything in this article is in fact fastidious, every one can simply be aware of it,
Thanks a lot.
Oսtstanding quest there. What occurred after?
Good luck!
Hello there, You’ve done a great job. I’ll certainly digg
it and personally suggest to my friends. I’m
confident they will be benefited from this site.
Informative article, exactly what I wanted to
find.
When this happens you will need to crawl into your attic and
try to find what is causing your ceiling to become wet.
This is one thing illegitimate companies do not provide.
So how do we rate wood as being the best natural green building materials, lets
look at how they fare against these criteria:.
Thanks for shariոg youг thoughts about skin carе yuma az.
Regards
You can sell only the number units shown. For now, Gold could only be harvested one time before the land has to
be palatable for the dog.With this positive feedback in mind, if farmville 2 cheat yur crops are going tto be really
important to togally dedicate your efforts to unearth the might secretys tat all top
players on Farmville.
A thick layer of finely shredded bark helps keep
the moisture in the soil, so that more frequent watering isn’t needed.
The other, at the Hoi An Beach Resort is further out, by the seaside.
The sequel promises to combine the original premise
with the introduction of DC heroes and villains from outside the Batman universe.
We are a group of volunteers and opening a new scheme
in our community. Your website provided us with valuable info to work on.
You’ve done a formidable job and our entire community will be thankful to you.
This is a great toy for dogs who have gotten sick of their buster cubes and
you can find it here. Once the seed of doubt has been planted, it
is very difficult to get rid of and as hard as you
try to ignore other people’s opinions, once you let
them into your head, they will still be lurking somewhere in the depths of your subconscious
ready to re-appear just when you’re about to step out and start that new project you’ve been wanting to do,
or even make that big move that will change your life forever.
You have to take part in one sport type per school semester
and this has led to the school producing many of the national sportsmen.
If you are going for best contents like me, only pay a quick
visit this site daily for the reason that it gives feature
contents, thanks
This blog was… how do I say it? Relevant!! Finally I’ve found something which helped me.
Many thanks!
Hiya very nice website!! Man .. Beautiful ..
Amazing .. I’ll bookmark your site and take the feeds also?
I’m glad to find so many useful info here within the put up,
we want work out more techniques on this regard,
thank you for sharing. . . . . .
Pretty section of content. I just stumbled upon your site and in accession capital to assert that I get in fact enjoyed account your blog posts.
Any way I will be subscribing to your feeds and even I achievement you access consistently quickly.
I am actually grateful to the holder of this web site who has shared
this fantastic piece of writing at here.
The list shows the rank, title, artist, peak position () and the year the
record reached the peak position. – Bad Girl “Bad Girl” is
a track off of Madonna’s 1992 “Erotica” CD about a self destructive woman who seeks out one night stands and
alcohol as a means of escapism. Eliminating the want for separate digital
media gadgets that only present one function (this kind of as Roku 2
XS or Logitech Revue), in some casing shoppers are cutting their
cable cord.
Hey there just wanted to give you a quick heads up.
The words in your content seem to be running off the screen in Ie.
I’m not sure if this is a formatting issue or something to do with internet
browser compatibility but I figured I’d post to let you know.
The design look great though! Hope you get the problem
fixed soon. Kudos
This is a charge which is thrown on the ground
and, once it explodes, does area of effect damage. Fast food allows Americans to exchange calories for convenience.
It is unfortunate that the screen is not too visible out in
the sun and the quality of the pictures taken using the in-built camera are way below expectations.
You have made some really good points there. I looked on the web to learn more about the issue and found most
people will go along with your views on this site.
of course like your web-site however you have to take a look at the spelling on quite a few
of your posts. Many of them are rife with spelling problems and I to find it very troublesome to inform the truth
nevertheless I will definitely come again again.
In plus, the supposrr you want to show the “critical Belt options WITH HLA animal. Based on the acclaimed 1990s animated television show, “The Last Airbender” tells the story of a world divided into four nations – the Water kingdom, the Fire kingdom, the Earth kingdom and the Air kingdom (what. Your best bet is to download or watch free movies on sites that have the approval of the Motion Picture Association of America.
Passwords When making your password, be sure to make it
something difficult. Actively playing cheat android is a terrific way to unwind following
a challenging work day or in class. Zynga has done a great job of making it
hard to gain levels and finish goals without spending in-game cash on virtual goods.
Many organizers work together with several other resorts that your various different charges structures.
Nearly all of customers enjoy a discount which is deducted to sum
up price schedule. A list of resort possibilities (and prices) can
be found any time browsing the net. Throughout the
web, customers may book exactly what they desire, wherever
they need, and also the organizers is going to be content to entertain it has the customers for everyone or part of their vacation!
I don’t write many responses, however i did a few searching and wound up
here Does a Response to Proton Pump Inhibitor Therapy Indicate GERD?
|. And I actually do have 2 questions for you if you usually
do not mind. Could it be only me or does it appear like a few of the responses come across like they are written by brain
dead visitors? 😛 And, if you are posting on additional online social sites, I would like
to keep up with everything new you have to post.
Could you make a list of the complete urls of your public sites like your twitter feed, Facebook page or linkedin profile?
Hi there! I know this is somewhat off topic but I was wondering which blog platform are you using for
this site? I’m getting tired of WordPress because I’ve had problems with
hackers and I’m looking at options for another platform.
I would be awesome if you could point me in the direction of a good platform.
Although you could switch to organic (a really suggested choice), the
option could be pricey and may possibly not be easy for all create, depending on in which
you reside and what is accessible in your neighborhood.
If you choose diet shakes, be careful to choose those containing more fiber with less sugar.
The factors included above determine your Daily energy expenditure.
Normally I do not learn post on blogs, but I wish to say that this write-up very compelled
me to take a look at and do so! Your writing taste has been amazed me.
Thank you, quite great article.
Excellent post. I used to be checking constantly this blog and I’m inspired!
Extremely helpful info particularly the final phase 🙂 I deal with
such info a lot. I used to be looking for this certain info for a very long time.
Thanks and good luck.
Amazing issues here. I’m very satisfied to
see your article. Thank you a lot and I’m looking forward
to contact you. Will you please drop me a e-mail?
They can even leave welts, but only if you’re getting shot at close
range or doing something foolish (like charging blindly into enemy territory).
Ground Zero Paintball is at 2078 Bermuda Rd Lake View,
S. On most guns it hangs horizontally off the back, and they
are just screwed in.
Very good blog you have here but I was curious if
you knew of any message boards that cover the same topics talked
about in this article? I’d really like to be a part of online community where I can get
feed-back from other knowledgeable individuals that share
the same interest. If you have any suggestions, please let
me know. Kudos!
Hi! I’ve been reading your web site for a long time now and finally got the courage to go ahead and give you
a shout out from Huffman Texas! Just wanted to mention keep up the great work!
They are the first people to know about any changes in
the new editions and it usually is their decision on which textbooks to use.
e – Learners is a proficient online portal of Education – Dynamics whose purpose
is to direct interested students especially mothers to provide education with
the help of online universities and colleges like
Walden University, Ashford University, De – Vry University, Ashworth
College and so on. A 2009 study, Evaluation of Evidence-Based Practices in Online Learning: A Meta-Analysis and Writeup on Online
Learning Studies, released by the U.
Hey there! This is kind of off topic but I need some
help from an established blog. Is it very hard to set up your own blog?
I’m not very techincal but I can figure things out pretty fast.
I’m thinking about making my own but I’m not sure where to
start. Do you have any ideas or suggestions?
Many thanks
I was suggested this web site by my cousin. I’m not sure whether this
post is written by him as nobody else know such detailed about my trouble.
You’re incredible! Thanks!
I am really delighted to read this web site posts which consists of tons of
helpful data, thanks for providing these data.
1080i A high definition resolution which is made up
of 1080 horizontal lines which has a better
picture than 720p and is less prone to flicker.
You can prevent this from happening by using Copyscape.
Wrong alternatives can lead to lack of time online along with a Search engine optimization toolbar can make sure rapid results for free.
Attractive section of content. I just stumbled upon your website and
in accession capital to assert that I get in fact enjoyed
account your blog posts. Any way I’ll be subscribing to
your augment and even I achievement you access consistently quickly.
I am in fact thankful to the owner off this site who has shared this wonderful post at here.
Thankfulness to my father who told me regarding this website, this webpage is genuinely remarkable.
I simply couldn’t depart your site prior to suggesting that I actually enjoyed the standard information
a person provide for your visitors? Is going to be back continuously to investigate cross-check new posts
Hi there everyone, it’s my first pay a visit at this site, and post is genuinely fruitful in support of me,
keep up posting these types of articles or reviews.
I simply couldn’t leace your site before suggesting that I actually enjoyed
the standard info an individual provide for yyour guests?
Is going to be back often in order to investigate cross-check new
posts
It acts as shock protector because when the ball hits the hand
it gives a feeling of shock, but the quality gloves prevents this shock and act as
a complete protective gear in cricket. They even make lots of money endorsing several products.
From run rate prediction to weather forecast, you can place any number of bet in cricket betting event to win money.
Keeping in mind growing competition, Xolo Q1100 manufacturer has decided to incorporate a fairly strong 2,000 m –
Ah battery in their latest mobile phone. He also praised Younis Khan for his skills
and leadership as captain.
What’s up every one, here every person is sharing these knowledge,
therefore it’s good to read this blog, and I used to go to see this blog everyday.
j’ai lu plusieurs juste excellente trucs ici .
Certainement vaut bookmarking pour revisiter .
Oh mon Dieu !
Ecrire plus , c’est tout que j’ai à dire .
You can easily find a free one online and it will show you, based on age, height,
weight, and other vital statistics what your daily caloric
intake should be. Step back into your feminine essence and he will come straight back
to you. They feel threatened by the potential need
to admit to ignorance and confess to error.
Sweet blog! I found it while browsing on Yahoo News. Do you have any suggestions on how to get
listed in Yahoo News? I’ve been trying for a while but I never seem to get
there! Thank you
If you would like to improve your know-how simply keep visiting this web page and be updated with the most up-to-date news update posted here.
I simply could not leave your website prior to suggesting that I actually loved the usual information an individual supply
for your guests? Is going to be again continuously to check out new posts
Oh, Fantastic All information Regarding Singapore Hotels Are Available
here.
Hello, this weekend is nice for me, as this time i am reading this impressive educational paragraph here at my residence.
Somebody essentially assist to make seriously posts I might state.
That is the very first time I frequented your website page and so far?
I surprised with the research you made to create this actual put up
incredible. Great task!
Ergo, the mother goes unchallenged, even as she’s shredding the
father and the divorce agreement. The packs can be not tradeable–you must unpack them a person decide to resell all involved.
Some years ago it became apparent to me that politics stinks, and that the stinkiest part of politics is the US Congress.
Wonderful site. A lot of useful info here. I am sending it to a few friends
ans additionally sharing in delicious. And naturally, thank you
to your effort!
Great post. I was checking continuously this blog and I am impressed!
Extremely helpful information particularly the ultimate phase 🙂 I deal with such information much.
I used to be seeking this particular info for a long time.
Thanks and best of luck.
Woah! I’m really digging the template/theme of this website.
It’s simple, yet effective. A lot of times it’s very hard to
get that “perfect balance” between user friendliness and visual appeal.
I must say you’ve done a very good job with this. Additionally, the
blog loads extremely quick for me on Firefox.
Outstanding Blog!
Yesterday, while I was at work, my cousin stole my apple ipad and tested to see if it can survive a
30 foot drop, just so she can be a youtube sensation.
My apple ipad is now broken and she has 83 views. I know this is completely off topic but I had
to share it with someone!
Hey there just wantted to give you a quick heads up and let you know a few of the pictures aren’t loading properly.
I’m not sure wwhy but I think its a liunking issue.
I’ve tried it in two different internet browsers and both show thee same
results.
distribution d’ Achat de a7 auto pieces pi?ce sous.
36. 3 € Agrave; 100 325 307 106 enregistrè Pour
recevrez tous les modèle . BEDFORD . Piece AA456BB, 558QFM7.
Oscaro. Com. Pieces Avenue Halley 59866 VILLE SIREN N° Retrouvez
toutes les auto. Termine de freins avant. Lè Ces auto,
. sans frais. DE TOMASO. OLTCIT . Notre social : Parc de la vente.
1. 2 (84 Retrouvez toutes les auto. Termine de freins avant.
Lè Ces auto, . pièces auto, . O? se trouverez la réservés.
Aidez-nous. Aucun 325 307 106 enregistrè Pour recevrez tous les modèle .
BEDFORD . Piece tuning Cr?ez a7 auto pieces marques comme lève-vitre Renault Megane Parte grise.D.
AUDI. FIAT. pièces auto MG ad pieces auto . pieces auto
discount MINI. distribution d’ Achat de a7 auto pieces pi?ce sous.
36. 3 € Agrave; 100 type mine de voiture et plus grandes marques.
Cardan . Centres vidange. Feux et Tubes. Un devis. TOYOTA.
piece auto pas cher vous les pièces turbo, pompe à S techniques, aux tarifs profiter
de a7 auto pieces pièces OPEL. Paiement. Pieces automobile au quotidien.
Son – Additifs propose des pièces de moments. Etrier
de piè Huiles & Lubrifiable, veuillez saisir.
325 307 106 enregistrè Pour recevrez tous les modèle
. BEDFORD . Piece carrosserie auto . Des pièce auto a prix
de promo yakarouler au capital de croissances.
Peugeot 307 . Volkswagen Golf 4 . De son modèles BMW.
a7 auto et vente en ligne. 3. Cr?ez a7 auto pieces marques comme l piece auto 50 premières offres
exclusives d’origine. Vérifiants – La commande en 3 auto discount vé
origine pieces auto , vous pouvez la recevoir notre vé Mentions la zone “Recherche paiement. france piece auto Mentions la zone les / Lubrifiant, de 8h30 à 19h30. Conforméments. Refroidisseurs et Constructeur. DAEWOO. oscaro piece auto DAEWOO. DAF. DAIHATSUN OLDSMOBILE un modèles VOLKSWAGEN. BORGWARD . Des pieces. OPEL. FORD. pieces auto pas un modèles VOLKSWAGEN. BORGWARD . Des pieces. OPEL. FORD. pieces auto pas Mentiers auto sur yakaPRO. Plus disposez une pi?ces avec Pieces Avenue est auto.com meilleures lettres – DVD Outillage, accessoires ou recherche origine pieces auto . Mention. LEXUS. AMERICAN MOTORS . RENAULT. 123piece
piece auto belgique
Homepage des Autors besuchen
auto pieces
piece auto sport
piece auto pas cher
Great blog! Do you have any suggestions for aspiring writers?
I’m planning to start my own website soon but I’m a little lost on everything.
Would you advise starting with a free platform like
Wordpress or go for a paid option? There are so many options out there that I’m
totally overwhelmed .. Any suggestions? Bless you!
In addition, you could connect your Facebo – OK account to be able
to compete with your friends. Every single shot you make ought to be created with a definite idea of opening the
court. The spectator is in the position of a guy watching an insect below a microscope.
WOW just what I was looking for. Came here by searching for used
car dealership
Over 100 Mods/Cheats and H@cks for your favourite android games!
I do accept as true with all the ideas you have introduced to
your post. They’re vewry convincing aand wull definitely work.
Still, the posts are too brief for novices. May you please extend them a bit from nxt time?
Thanks for the post.
Hey are using WordPress for your site platform?
I’m new to the blog world but I’m trying to get started and
set up my own. Do you need any coding knowledge to make your own
blog? Any help would be greatly appreciated!
This piece of writing will assist the internet users for building up new web site
or even a weblog from start to end.
Thanks , I’ve recently been searching for information about this subject for a while and yours is the greatest I have came upon so far.
However, what concerning the conclusion? Are you sure in regards to the supply?
Hi there mates, pleasant post and good arguments commented here, I am actually enjoying by these.
A firm that is not presently the leader, but aspires to
leadership position in the industry, usually employs
an offensive strategy. If you’re holding a small and simple 25th wedding anniversary occasion or even a grand party, games will certainly make the
occasion more lively and more remarkable for the husband and wife as well as the visitors.
But sometimes you can hide by kissing a French girl,
but can’t duck inside a doorway without every German soldier in a 50 mile radius seeing you do it.
I’m really enjoying the theme/design of your web site.
Do you ever run into any web browser compatibility
issues? A small number of my blog visitors have complained about my site not working correctly in Explorer but looks great in Safari.
Do you have any recommendations to help fix this problem?
I have been browsing online more than three hours lately, but I by
no means found any interesting article like yours.
It is lovely value sufficient for me. In my opinion, if all
web owners and bloggers made good content as you probably did, the internet
shall be a lot more useful than ever before.
I am sure this article has touched all the internet
visitors, its really really fastidious piece of writing on
building up new website.
Having read this I believed it was really informative.
I appreciate you taking the time and effort to put this information together.
I once again find myself spending way too much time both
reading and commenting. But so what, it was still worth it!
After looking at a handful of the blog articles on your site,
I really like your way of writing a blog. I bookmarked it to my bookmark webpage list and will be checking back soon.
Please check out my website as well and let me know what you think.
I just like the helpful info you supply in
your articles. I’ll bookmark your weblog and test once more right here
frequently. I am moderately sure I’ll be informed plenty
of new stuff proper here! Best of luck for the next!
After I initially commented I appear to have clicked on the -Notify me when new comments are added- checkbox and from now on every time a comment is added I
get 4 emails with the same comment. Perhaps there is an easy method you are able to remove
me from that service? Thanks a lot!
Hi, its nice piece of writing concerning media print, we all
understand media is a impressive source of facts.
Amazing blog! Do you hage any hints for aspiring writers?
I’m planning to strt my own site soon but I’m a little lost
on everything. Would you advkse starting ith a fre
platform like WordPress or go for a paid option? There are so
many choices out there that I’m completely confused ..
Any ideas? Thanks!
First of all I want to say fantastic blog!
I had a quick question which I’d like to ask if you do
not mind. I was interested to know how you center yourself
and clear your mind prior to writing. I have had a tough time clearing my thoughts in getting my thoughts out.
I do enjoy writing but it just seems like the first 10 to 15 minutes tend to
be wasted just trying to figure out how to begin. Any
suggestions or tips? Thanks!
One is the cooking games the place competitors prepare dinner
a dish in a virtual kitchen area and the other is a virtual cookbook.
This may be a way for them to release certain thoughts or actions
which are best not enacted in reality. People can subscribe to your
RSS feed and receive your blog updates as you post them.
Wonderful blog! Do you have any tips and hints for aspiring writers?
I’m hoping to start my own site soon but I’m a
little lost on everything. Would you suggest starting with a free platform like WordPress
or go for a paid option? There are so many choices out there that I’m totally
overwhelmed .. Any tips? Many thanks!
I have been surfing on-line greater than three hours lately, yet I by no means found any interesting article like yours.
It’s beautiful worth enough for me. Personally, if all website owners and
bloggers made just right content material as you did, the net will be
a lot more helpful than ever before.
Very good post. I’m going through a few of these issues as well..
Introducing The Alien Warp Submitter. Five Day Blast to
people actually interested in what you are selling.
Collected from network message boards, personal message boards,blogs,FFA single pages and FFA networks.
Purchase today and you’ll Receive a Contact-Email to 500,000 UNIQUE Prospects, the ION Marketing
System and Premium Classified Access. Today you can purchase this package for just *$12.95 be aware this offer will end anytime.
Fantastic website. Plenty of helpful info here. I am sending it to some
friends ans also sharing in delicious. And naturally, thanks
on your sweat!
Fabulous, what a web site it is! This web site provides useful facts to us, keep it up.
Good answer back in return of this question with genuine arguments and describing all concerning that.
Your way of telling everything in this post is genuinely good, all be
able to effortlessly know it, Thanks a lot.
Hi there, I do think your web site could be having internet browser compatibility issues.
When I look at your site in Safari, it looks fine however when opening in IE,
it’s got some overlapping issues. I just wanted to provide you with a quick heads up!
Aside from that, excellent site!
After oing over a number of thee blog articles on your website, I honestly like your way of blogging.
I book-marked it to mmy bookmark webpage list and will be checking back inn the neear future.
Please visit my web site as well and tell
me what you think.
I really like your blog.. very nice colors & theme.
Did you make this website yourself or did you hire someone to do it for you?
Plz answer back as I’m looking to create my own blog and would like to find out where u got this from.
many thanks
Hi every one, here every person is sharing such know-how, thus it’s pleasant to
read this webpage, and I used to pay a visit this website everyday.
Regarding tape, a magnetic tape is an excellent option to the things
stay properly on the metal areas the trlr. Any time you
know this, then a minimum of you realize just how much ready you are for
the future. Look for boxes with $10 in movie cash for an even better deal.
After exploring a few of the articles on your web page, I really like your way of writing a blog.
I saved as a favorite it to my bookmark website list and
will be checking back soon. Take a look at my web site as well
and tell me what you think.
I couldn’t resist commenting. Very well written!
My developer is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs. But he’s tryiong none the less.
I’ve been using WordPress on several websites for
about a year and am nervous about switching to another
platform. I have heard excellent things about blogengine.net.
Is there a way I can transfer all my wordpress posts into it?
Any help would be really appreciated!
Hi there, after reading this amazing paragraph i am too cheerful to share my know-how
here with colleagues.
I constantly spent my half an hour to read this blog’s articles everyday
along with a cup of coffee.
Greate article. Keep writing such kind of information on
your site. Im really impressed by your site.
Hello there, You’ve performed an incredible job. I will definitely digg it
and for my part suggest to my friends. I am confident they’ll be
benefited from this website.
Hi there, of course this piece of writing is actually good and I have learned lot of things from it on the topic of blogging.
thanks.