
Researchers have found markers to identify patients with Barrett’s esophagus (BE) at greatest risk of developing esophageal adenocarcinoma. These are described in the August issue of Clinical Gastroenterology and Hepatology.
In patients with BE, part of the normal stratified squamous epithelium of the lower esophagus is replaced with metaplastic columnar epithelium that contains goblet cells (see below figure).
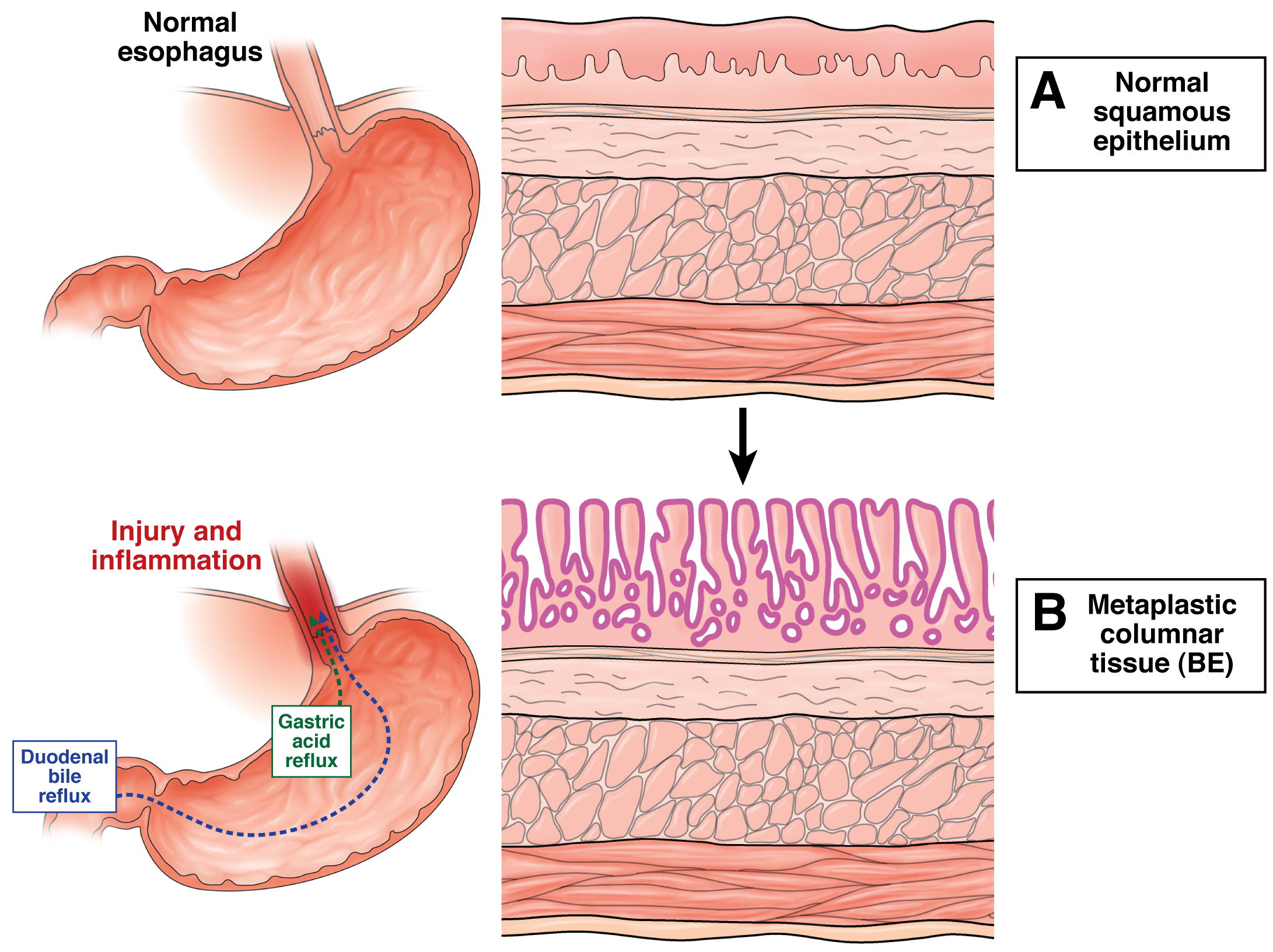
In BE, injury and inflammation in the esophagus causes part of the normal squamous epithelium to be replaced by metaplastic columnar tissue, increasing the risk for cancer.
Patients with BE are at increased risk of developing esophageal adenocarcinoma, compared with the general population. However, the absolute incidence of this cancer is relatively low (estimates range from 0.1% to 0.7% per year).
It is therefore a challenge to identify the small subpopulation of patients whose BE will progress to cancer. Most patients undergo long-term endoscopic surveillance to identify cancer early, when it is treatable. However, identification of biomarkers and other factors that determine patients’ cancer risk could reduce the costs, risks, and inconvenience of long-term surveillance.
Catherine Duggan et al. measured insulin sensitivity and other markers of obesity and metabolic syndrome, which have been associated with BE, in 392 patients enrolled in the Seattle Barrett’s Esophagus Study. The authors collected data on the patients for more than 7 years, and then evaluated the association between these factors and development of esophageal adenocarcinoma.
They associated insulin resistance and increased concentrations of leptin in fasting plasma samples with risk for progression to esophageal adenocarcinoma. These associations were strongest among men, within the first 6 years of follow-up evaluation, and among patients who were not insulin resistant when they were diagnosed with BE but developed resistance later.
Neither insulin resistance nor insulin levels have been evaluated risk factors for progression of BE to esophageal adenocarcinoma, although a recent study did report that diabetic individuals were at increased risk for this cancer, compared to people without diabetes.
Duggan et al. propose that increased circulating levels of insulin could contribute to tumorigenesis by altering various cancer-associated signaling pathways.
Leptin is an adipokine that regulates food intake and energy expenditure. Levels of leptin are increased in obese individuals, and levels of leptin receptor in patients with esophageal adenocarcinoma have been associated with advanced tumor stage.
Duggan et al. also observed an inverse association between levels of adiponectin and the risk of esophageal adenocarcinoma.
Adiponectin is a peptide hormone that circulates in high-, medium-, and low-molecular-weight forms; its levels are inversely correlated with body mass index. Decreased levels of the high-molecular weight form correlate with insulin resistance; this form is down-regulated in overweight and obese patients. Studies have shown that adiponectin increases apoptosis and inhibits leptin-induced proliferation in esophageal cancer cell lines.
Duggan et al. conclude that increased levels of leptin and insulin resistance might be used to identify patients with BE at greatest risk for cancer, whereas patients with increased levels of high-molecular-weight adiponectin could be at lower risk.
Although further studies are required to confirm these findings, the authors state that insulin levels might be decreased successfully via behavioral and lifestyle changes such as increasing physical activity to reduce BE patients’ risk of progression to esophageal cancer.
More Information on Barrett’s Esophagus
Read the article online.
Duggan C, Onstad L, Hardikar S, et al. Association between markers of obesity and progression from Barrett’s esophagus to esophageal adenocarcinoma. Clin Gastroenterol Hepatol 2013;11:934–943.


Pingback: Which Patients With Barrett’s Esophagus Will Develop Esophageal Cancer? | The Salgi Foundation
Link exchange is nothing else except it is simply placing the other person’s
weblog link on your page at suitable place and other person
will also do same in favor of you.
Great info. Can meassuring levels of good bacteria and putting a person on probitotic solve the issue sometimes ? And also making sure that person doesn’t have chronic constipation which from what I understand, and please correct me if I am wrong, can cause constipation ? Can those factors be the reason or cause ?
Great Information about Barretts Esophagus. Keep posting
We are at Healing Touristry an ISO Certified 9001:2015 Indian healthcare service provider that offers medical treatment to foreign nationals, seeking affordable and safe medical tourism facilities… Click here https://www.healingtouristry.com/